Tos cronica y esputo purulento ¿Cómo detectar bronquiectasia?
feb 26, 2026
Author: Jin Jianmin, Chief Physician at Tongren Hospital of Capital Medical University, Beijing.
Reviewer: Zhang Haicheng, Chief Physician at Peking University People's Hospital.
Chronic bronchiectasis is not the same as chronic obstructive pulmonary disease; distinguishing between these concepts is the first step in understanding this respiratory condition.
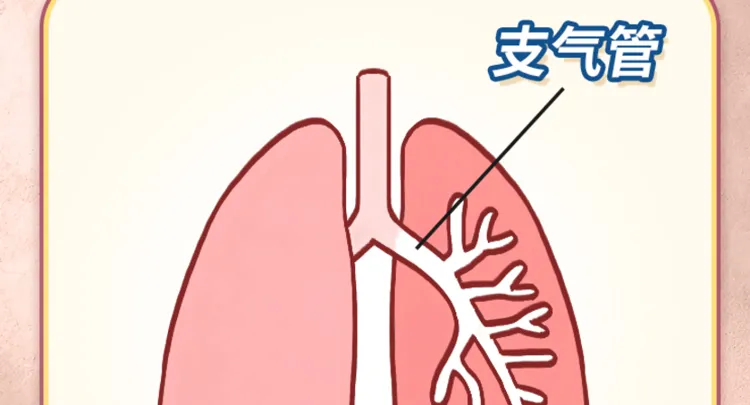
Bronchiectasis is an anatomical concept often seen in CT scan reports. It refers to an abnormal widening of the bronchial lumen that exceeds the normal diameter. Simply put, our trachea and bronchi resemble a tree, branching hierarchically into thinner forms. In the bronchial area, for various reasons, the lumen becomes enlarged, a condition known as bronchiectasis. Therefore, it is fundamentally a change in the bronchopulmonary structure.
Figure 1 Original image copyright, reproduction unauthorized.
Bronchiectasis is an independent primary disease. Patients with bronchiectasis will necessarily show signs of bronchial dilation on a CT scan. However, not everyone with visible bronchial dilation on a CT scan has bronchiectasis. This is because many other diseases, such as pulmonary interstitial fibrosis with traction bronchiectasis or the sequelae of tuberculosis, can also cause bronchial dilation, and this dilation is not an independent disease, but rather an "associated result" of the primary disease.
However, in reality, doctors often refer to 'bronchiectasis' simply as 'bronchiectasis.' So when a patient asks 'What illness do I have?', the doctor may commonly say 'you have bronchiectasis.' In this case, what the doctor refers to as 'bronchiectasis' generally indicates the condition known as 'bronchiectasis.'
Bronchiectasis is a chronic infectious disease of the airways, primarily characterized by recurrent cough, production of large amounts of purulent sputum, and sometimes hemoptysis. The key to diagnosis lies in the features observed in high-resolution computed tomography (HRCT) of the lungs. Currently, there are no very precise statistics on its incidence. According to foreign documents, the incidence of bronchiectasis in adults in the United States is approximately 52 per 100,000, although these are old data when high-resolution CT was not yet widely used. In this country, bronchiectasis does not receive the same attention as asthma and chronic obstructive pulmonary disease (COPD), so there is also a lack of information about its national incidence.
The pathogenesis of bronchiectasis revolves around the interaction between bronchopulmonary infection and bronchial obstruction, forming a vicious cycle.
Under normal physiological conditions, respiratory secretions can be easily cleared through mechanisms such as ciliary beating. However, once inflammation occurs in the airways, secretions increase significantly; if bronchial obstruction also occurs, mucus cannot be adequately expelled and accumulates in the bronchi. This accumulation of mucus can exacerbate airway obstruction and induce more severe inflammation, damaging supporting structures such as smooth muscle and elastic fibers of the bronchial wall. This cycle of 'infection-obstruction-new infection' repeats, which can lead to persistent and irreversible bronchial dilation, eventually developing into bronchiectasis.
The causes of bronchiectasis can be categorized into the following types: 1. Genetic factors: Certain hereditary diseases such as cystic fibrosis and bronchiectasis associated with other conditions might lead to bronchiectasis. 2. Infection: Repeated respiratory infections, especially severe pneumonia or bronchitis during childhood, can result in bronchial damage. 3. Foreign body inhalation: The inhalation of foreign objects can lead to bronchial obstruction and inflammation, resulting in dilation. 4. Environmental factors: Prolonged exposure to harmful gases, smoke, or other irritants may cause chronic bronchial inflammation, promoting the development of dilation. 5. Immunodeficiency: Patients with abnormalities or deficiencies in the immune system are more susceptible to infections, which can lead to bronchiectasis. These causes are often interconnected when leading to bronchiectasis and need to be considered comprehensively.
Firstly, bronchopulmonary infection is the primary cause. Infections caused by various pathogens can lead to inflammation, with common bacteria including Haemophilus influenzae, Klebsiella pneumoniae, and Pseudomonas aeruginosa. Regarding viruses, the measles virus is also quite common; many patients suffered from this illness in childhood and may develop bronchiectasis in adulthood. Furthermore, infection with non-tuberculous mycobacteria is also a significant cause.
Secondly, there is bronchial blockage. For instance, when a foreign body obstructs the airways, the distal lung tissue may develop obstructive pneumonia. If inflammatory secretions cannot be cleared, this could lead to localized bronchiectasis. Fortunately, this type of cause is usually reversible; if the foreign body can be removed in time, the associated bronchiectasis may improve.
Additionally, the disorder of ciliary movement in the airways is another cause. The cilia in the airways normally move rhythmically to eliminate secretions. If ciliary movement is abnormal, ceases, or moves erratically, secretions accumulate in the airways, potentially triggering and exacerbating bronchiectasis. Related diseases include situs inversus syndrome and Kartagener syndrome, among others.
Finally, genetic diseases such as congenital abnormalities of the bronchial wall development and alpha-1 antitrypsin deficiency may also lead to bronchiectasis.
Understanding these basic concepts helps patients and their families have a clearer view of the nature of bronchiectasis, differentiating between 'bronchiectasis' and 'dilated bronchial disease.' This also enables a more precise understanding of disease progression. In this way, when communicating with the doctor about the disease status and discussing treatment options, information can be exchanged more efficiently, facilitating cooperation in disease treatment and management.
#salud
#pulmonar


© 2025 Tribu Salud.